

For some, the call to serve is impossible to ignore.
For Robin Richardson, a registered nurse at Central Peninsula Hospital, that call took her to New York’s White Plains Hospital in Westchester County, where she spent six weeks caring for critically ill COVID-19 patients.
Despite having 30 years nursing experience in emergency rooms and intensive care units, Richardson said that the time she spent at the heart of the COVID-19 pandemic was an experience unlike any other.
“It’s not like I’ve been an ICU nurse for five minutes,” Richardson said. “I’ve been doing this long enough … I mean I’ve seen some horrible things, and this, psychologically, was very different. Very very different.”
Richardson spoke to the Clarion on Friday about how she ended up in New York during the height of the pandemic, what her time at White Plains was like and what lessons she brought with her back to Alaska.
The call to action
Richardson has been working at Central Peninsula Hospital in Soldotna since 2016, when she was hired to be the ICU supervisor. A couple of years ago Richardson transitioned to the cardiac rehabilitation unit at the hospital. After 30 years doing emergency and intensive care she was ready for something slightly less stressful, she said.
“It’s a very happy job all the time because people are motivated to get better and improve themselves,” Richardson said of cardiac rehab. “And so I thought that would be a great change for me, to get me away from the drama of trauma.”
Then in March of this year the COVID-19 pandemic hit, and hospitals around the state — including CPH — prepared for the worst. Elective procedures — including cardiac rehab, Richardson’s current department — were put on hold. Nurses from elective departments were cross-trained for ICU work and entire sections of the hospital were designated for COVID-19 treatment.
“Basically, everybody was kind of on a standby,” Richardson said. “Like we were waiting for the floodgates to open and all these intubated and critical COVID patients come in, but, thank God, we have not seen that yet.”
Richardson found herself without any patients and with nowhere to put her years of experience to use. Meanwhile, she was hearing about the struggles of nurses around the country dealing with outbreaks of severely ill patients in densely populated areas.
“I thought, you know, it’s just crazy that I’ve got 31 years of critical care experience, and I’m not doing anything with it,” Richardson said. “There’s patients dying and nurses absolutely pulling their hair out and crying in the corner that need help, and I’m sitting down here, really not using my skills. I even thought about if I could be used somewhere else in Alaska, and really there wasn’t the need. So I just decided that I would probably be of some value if I went to maybe the worst spot possible to see if I could help.”
Working in coordination with Central Peninsula Hospital and a company called Medical Solutions, Richardson was able to secure a six-week shift at White Plains Hospital just outside of New York City and was given a two-month leave of absence from CPH. On April 19, she landed in a mostly empty terminal at JFK International Airport, unsure of what she was about to face.
“I’ve been to JFK years ago,” Richardson said. “It’s kind of a madhouse, you know. Ginormous airport and all that. And my voice was echoing, talking to myself. All the luggage carousels were empty. There was myself and six people flying from Seattle to JFK on the plane.”
Fighting the pandemic
On her first day, Richardson was temperature-checked and given some N95 respirator masks at the entrance of the hospital and told to report to the ambulatory surgery area. There, a separate room was designated for donning all of the necessary personal protective equipment (PPE): a PAPR respirator mask, disposable head cap, gloves, feet covers, leg covers and a heavy plastic gown that came down past the knees.
“They (the gowns) were the consistency of shower curtains, I kid you not,” Richardson said. “I thought, if I have to go pee, this is going to be a 30-minute adventure.”
Richardson said that almost every unit of White Plains Hospital had been converted into a COVID-19 ICU unit. Richardson was working the night shift three to four times a week in what used to be the endoscopy unit of the hospital, where as many as 36 patients were being intubated on ventilators at any given time.
Over the course of her six weeks in New York, Richardson cared for 53 critically ill COVID-19 patients. Only two of those patients lived.
“That goes completely against a critical care nurse’s job,” Richardson said. “When you’re in a critical care area, you go in every day to save someone’s life. I’m not helping you through the process of dying. That’s not my job. My job is to save you.”
After the first week, Richardson said, she began marking down a fraction on a piece of paper when she got home each day.
“Blank over blank: the number that I took care of and the number that died. I did this throughout my day, and it’s awful. It’s awful. I’ve taken care of incredibly ill patients in my career. The difference with this is the speed in which the patient goes from walking into the emergency room with ‘I don’t feel good’ to death. That’s the difference.”
Richardson’s patients, for the most part, did not fall under the populations considered particularly vulnerable to the disease: the elderly and those with underlying health conditions. At 55, Richardson said she was older than about half of the patients she treated, and few of them had any “comorbidities” beyond being diabetic or having low blood pressure.
“I had a 41-year-old mother of four, and the only medication she took was birth control,” Richardson said. “Like, nothing was wrong with this person. … These were your average working people that had been sick three to five days and came to the ER.”
Richardson explained that one of the challenges with critical COVID-19 patients is that, when the body is that ill and organs can’t function properly, blood levels become imbalanced. This leads to blood clots forming, which can cause heart attacks or strokes. The speed of the “clotting cascade” that occurs in critical COVID-19 patients is unlike anything Richardson had dealt with before.
To prevent clotting, nurses administer a blood thinner called heparin via an IV drip. Richardson explained that heparin is used commonly for patients needing an anticoagulant, but its use is heavily regulated. With COVID-19 patients, Richardson said that they often had to administer way more of the drug than they ever would in an attempt to keep their blood levels under control, and often to no avail. It was common for a COVID-19 patient in Richardson’s unit to be in full kidney failure within 24 hours of admission, she said.
The pneumonia caused by COVID-19 was also unlike anything Richardson had seen before. Patients lay on their stomachs for about 16 hours a day to allow the lungs more room to breathe, and there was a team of physicians whose job was to turn these patients over periodically to allow them to rest.
Dialysis, induced comas and antifungal medications are just a few of the treatments Richards described when walking through what it was like to care for someone in that condition. Then there is the added challenge of forcing these patients to be isolated from their families.
There were a few cellphones available in each unit, Richardson said, that families could call to speak to their loved ones. Most of the patients were comatose and couldn’t speak back, but the families on the other end of the line could speak for as long as they wanted. There was also one iPad per unit which families could “reserve” for a time slot to video chat, but that was only if there was a spare nurse available to hold the tablet in front of the patient.
Richardson had to make many calls to family members with bad news, and the families were often confused as to how their loved one could have died so quickly.
“As a nurse, I took that for granted,” Richardson said. “I didn’t think about the fact that these people are dropping off their loved ones, and they’re not going to see them again.”
Even the two patients under Richardson’s care who survived the disease have a long road to recovery ahead of them. Both ended up breathing and eating through a tube, and will likely have to go through months of therapy to learn how to walk again. Richardson recalled seeing and speaking with one of the survivors, a young married man, on her last day at work. She noticed that he looked ready to give up, and he acknowledged he was.
“I called him by his name and I grabbed his chin a little bit and I said, look at me,” Richardson said. “You are my hero. All of these patients that have died are counting on you not to die. You’ve got to make it out of this unit. You have to, and you know it. … If you survived all what you’ve gone through, you can survive this last part.”
Coming home
Richardson was required to quarantine for two weeks upon returning to Alaska. Luckily, she and her husband had recently bought a boat that was docked in Sitka, so she spent her quarantine on the open water on her way back to Soldotna. Richardson has resumed her position in the cardiac rehab unit at CPH, where patients are being accepted under strict COVID-19 mitigation policies.
Alaska has had 72 hospitalizations of COVID-19 patients since the start of the outbreak, which is only about 20 more than Richardson treated on her own in New York. Alaska’s geography and low population density may mean that the outbreak does not become as severe as it has in the Lower 48, Richardson said, and Alaskans should consider themselves lucky in that regard.
“Obviously we don’t have the criticality that they’re having in other areas, but you know we don’t have as much of a population either,” Richardson said. “Do I think that it’s possible that it’s going to come up here? It’s possible. Anything’s possible. Do I think it’s political? 100% no, I don’t.”

Robin Richardson, RN at Central Peninsula Hospital in Soldotna, is seen here in full personal protective equipment during her shift at White Plains Hospital in White Plains, New York on May 1, 2020. (Photo courtesy Robin Richardson)

Empty streets outside White Plains Hospital are seen here in White Plains, New York on April 22, 2020. (Photo courtesy Robin Richardson)
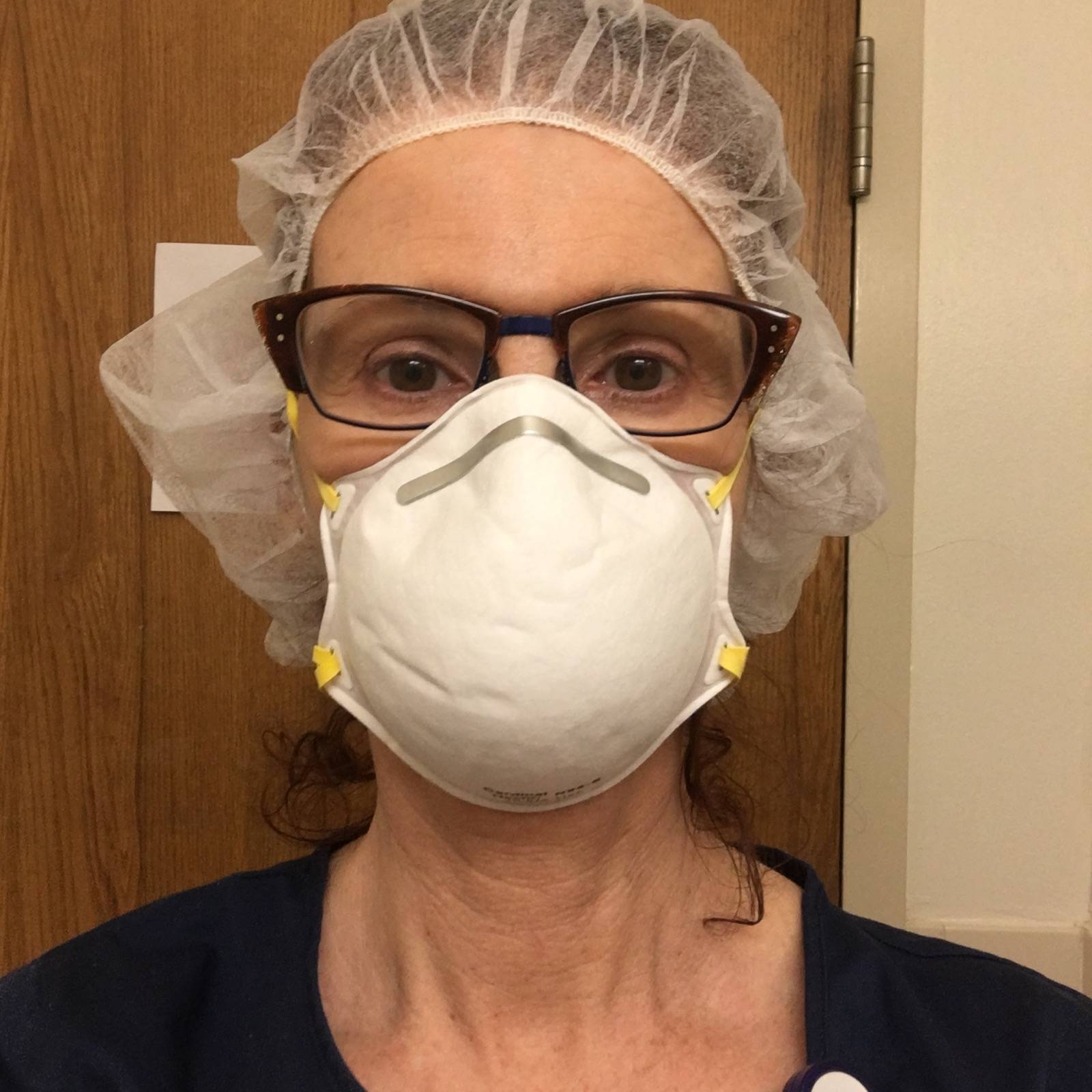
Robin Richardson, an RN at Central Peninsula Hospital in Soldotna, gets ready to don her personal protective equipment during a shift at White Plains Hospital in White Plains, New York on May 3, 2020. (Photo courtesy Robin Richardson)

The empty terminal at JFK International Airport in New York City is seen here on April 19, 2020. (Photo courtesy Robin Richardson)
The empty terminal at JFK International Airport in New York City is seen here on April 19, 2020. (Photo courtesy Robin Richardson)
